Femoroacetabular Impingement (FAI) is a hip and groin pain condition common in younger, athletic populations, particularly prevalent in the 18 to 35 year old age group [1].
This disorder is caused by premature contact of the acetabulum (hip socket) with the proximal head and neck (the ball of our hip) of the femur during certain movements [2]. FAI is generally characterised by deep seated, intermittent discomfort in the hip and groin areas, which can present as both a deep ache during and after activity, and occasionally a sharper pain in more aggravating positions such as sitting cross legged or when changing direction [3]. The condition is more common in sports or activities that require quick and repeated acceleration [4]. In addition to this primary symptom, pain can also be felt in the buttock, back and anterior thigh [3].
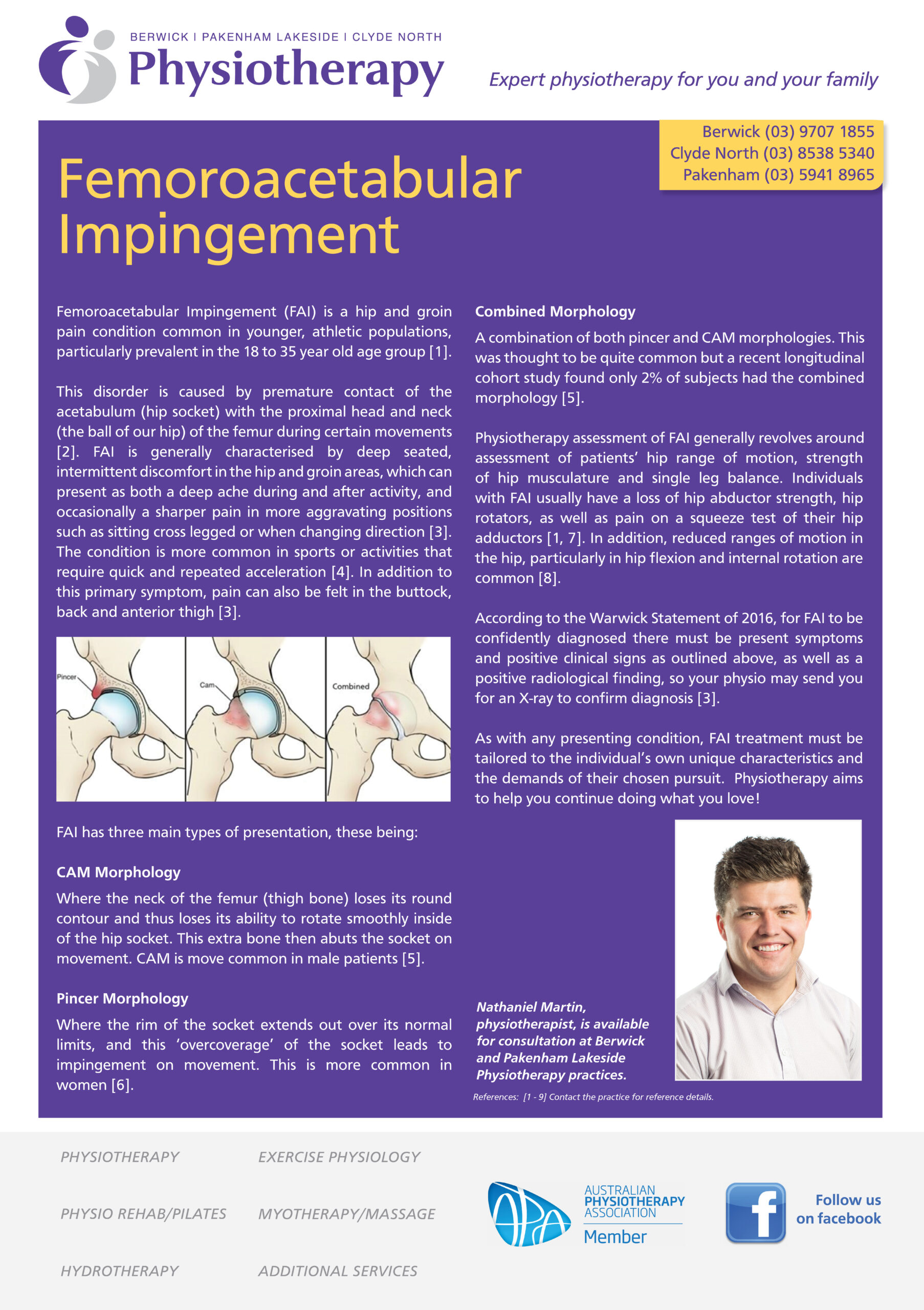
FAI has three main types of presentation, these being:
CAM Morphology
Where the neck of the femur (thigh bone) loses its round contour and thus loses its ability to rotate smoothly inside of the hip socket. This extra bone then abuts the socket on movement. CAM is move common in male patients [5].
Pincer Morphology
Where the rim of the socket extends out over its normal limits, and this ‘overcoverage’ of the socket leads to impingement on movement. This is more common in women [6].
Combined Morphology
A combination of both pincer and CAM morphologies. This was thought to be quite common but a recent longitudinal cohort study found only 2% of subjects had the combined morphology [5].
Physiotherapy assessment of FAI generally revolves around assessment of patients’ hip range of motion, strength of hip musculature and single leg balance. Individuals with FAI usually have a loss of hip abductor strength, hip rotators, as well as pain on a squeeze test of their hip adductors [1, 7]. In addition, reduced ranges of motion in the hip, particularly in hip flexion and internal rotation are common [8].
According to the Warwick Statement of 2016, for FAI to be confidently diagnosed there must be present symptoms and positive clinical signs as outlined above, as well as a positive radiological finding, so your physio may send you for an X-ray to confirm diagnosis [3].
As with any presenting condition, FAI treatment must be tailored to the individual’s own unique characteristics and the demands of their chosen pursuit. Physiotherapy aims to help you continue doing what you love!